Identify the basic structures and functions of the digestive (gastrointestinal) system, including the five main functions. Be able to name the major parts of the GI system and tell what they do.
Define the symptoms of gastrointestinal disorders.
Describe the major gastrointestinal disorders for which medications are prescribed.
Describe the actions, give examples, nursing care and side effects for these drug groups:
antacids
antisecretory drugs
digestants
antiflatulents
emetics
antiemetics
anticholinergics
antispasmodics
diarrhea medications (Discuss non-drug means of controlling diarrhea and
for preventing constipation)
cathartics (laxatives and purgatives)
antiparasitics
Identify principles to remember in administering medications for the digestive system safely.
Gastrointestinal (G.I.) system-alimentary or digestive system anatomy and physiology.
Refer to your textbook pg 337
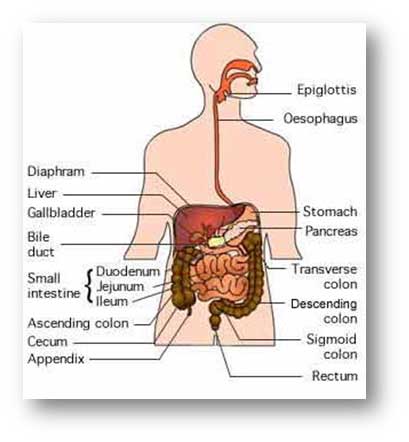
Structures
Mouth-Digestion begins in the mouth. Food is broken into smaller pieces, mashed and mixed with saliva.
Esophagus-muscular tube extending from the pharynx to the stomach. About nine inches in length. Food passes through the GI system with the assistance of a wavelike process called peristalsis.
Stomach-muscular, pouch-like distensible portion of the alimentary canal below the esophagus and below the diaphragm. The opening from the esophagus is the fundus and the opening into the small intestine is the pylorus. Made up of four layers of tissue, primarily muscular and mucous lining.
Secretes gastric juice and converts proteins.
Acts as a reservoir, moderating the movement of contents into the next portion of the alimentary canal. Acid kills microorganisms. Limited ability to absorb nutrients.
Expands to hold up to 2000 ml/2 quarts of food.
Food may stay in the stomach for about 3 hours.
Small intestine-extends from the stomach, into the duodenum (about 10 inches long) connecting to the jejunum (about 8 feet long) which then joins the ileum (about 12 feet long).
Duodenum receives food through the pyloric valve of the stomach.
Receives secretions from the liver and pancreas which aid digestion in the first third of the small intestine.
Wall has glands, blood and lymph vessels, nodules, folded surface and tiny finger-like projections called villi that absorb products of digestion.
Absorption of nutrients and medications occurs in the alkaline environment of the last 2/3 of the small intestine and are transported to the liver via the bloodstream.
Large intestine-also called the colon (about 5 feet 100ig). Consists of the cecum, ascending, transverse, descending, and sigmoid colon, the rectum, and the anus.
Primary function is to absorb water from digestive byproducts.
Produces feces.
Rectum-end of the large intestine; holds feces. Centers for defecation reflex are in the medulla and 2nd, 3'd, and 4th sacral segments.
Anus--Opening at the far end of the intestine for expelling feces.
Liver-secretes digestive substances (bile-aids in digesting fats), removes certain waste products from the blood.
Produces clotting factors and some immune factors.
Breaks down and inactivates many drugs and toxins.
Nutrients are stored in the liver and are released into the blood stream as needed by the body.
Gallbladder-a pear-shaped storage pouch on the undersurface of the right lobe of the liver.
Holds bile until it is discharged for digestion.
Pancreas--secretes digestive substances into the digestive tract and insulin into the bloodstream. It is a gland with its head attached to the duodenum and its tail portion reaches toward the spleen. Pancreatic juice plays an important role in digestion breaking fats, proteins, and carbohydrates into particles that can be absorbed.
Produces internal and external secretions.
Hormones are produced including insulin and glucagon. These work with hormones from other endocrine glands to regulate carbohydrate metabolism. Diminished secretion of insulin by the islets of Langerhans results in diabetes mellitus.
Major functions
Breaking up food into smaller pieces
Transporting food through the GI tract-peristalsis
Mechanisms of digestion and elimination-Peristalsis and the secretion of digestive enzymes are under the control of the autonomic nervous system, so digestion is affected by stress. Normal bowel elimination is from 3 times per day to every 3 days.
Click on views of the digestive systems: Click Here
Disorders of the GI digestive system
Refer to your textbook pg 339
Video on Gastrointestinal System Disorders Part 1 Click Here
Video on Gastrointestinal System Disorders Part 2 Click Here
Symptoms-changes in normal process of digestion.
Emesis or vomiting- reverse peristalsis. Expelling stomach contents through the esophagus and mouth and/or nose.
Nausea-feeling or need to vomit. May or may not precede vomiting.
Constipation-failure to have regular bowel movements due to hardened feces, slow peristalsis movement of the intestine, lack of bulk in the diet, psychological factors, or lack of physical activity.
Heartburn-acid liquid reflux from the stomach into the esophagus causing a "burning" feeling in the chest. Has no relation to heart other than location of the pain in upper chest area.
Abdominal cramps-tightening, "cramping" feeling in the alimentary canal. May be in the upper or lower colon.
Eructation-belching; expelling gas or air from stomach through esophagus.
Flatus-gas in the GI tract, expelled through the anus.
Diarrhea-loose watery stools or too frequent stools. Can be caused by greasy food or too spicy food, coffee or other intestinal irritants.
Increased intestinal motility-moving food through the intestine with too much speed. Affected by nervous tension, infections, drugs, etc.
Tarry stools-dark, black, sticky consistency. Can be a sign of GI bleeding or may be side effect of iron supplements.
Anorexia-lack of appetite.
Tooth and gum disorders-residents may avoid foods that are hard to chew, such as fruits and vegetables or foods high in bulk and fiber, leading to other GI problems. Refer to your textbook pg 341
Gastritis-inflammation of stomach, characterized by pain, tenderness, nausea, vomiting.
Diseases and disorders of the GI/Digestive system Refer to your textbook pg 341
Ulcers - an erosion o the lining of the stomach or duodenum. Underlying tissue is exposed. Hypersecretion of stomach acids has been thought to be the main cause. Current evidence shows that there are other underlying causes: disruption in the normal mucosal defense and repair, increasing susceptibility to breakdown by stomach acid. Acids destroy tissue. Infections and medications may destroy stomach lining.
Related medication and treatment:
Antibiotics
Antacids
Anti-secretory drugs
Dietary changes-eliminate foods that cause resident distress. Diet changes overall do little to promote healing.
Liver disorders-Liver is the largest and most metabolically complex organ. Symptoms are result of changes in cell function or impaired bile secretion. Refer to your textbook pg 342
Clinical features of liver disease include:
Jaundice-yellowing of the skin and sclera, dark urine. Bilirubin builds up in tissues rather than metabolized. Many causes for bilirubin to increase in bloodstream and eventually tissues, including secretory or metabolic malfunctions.
Hepatitis-general inflammation or infection of the liver. Viral types are classified as Hepatitis "A,” “ B," "C" etc. Refer to your textbook pg 342
Cirrhosis-liver damage that results in the liver becoming fibrous, scarred and forming nodules. Many things may cause cirrhosis-chronic hepatitis, infections, toxins, changes in immune response, biliary obstruction, diabetes mellitus, and poor nutrition. It is the "end-stage" of many forms of liver injury, including chronic alcoholism. Hepatitis and Cirrhosis video Click Here
Gallbladder disorders- Refer to your textbook pg 343
Cholecystitis-inflammation of the gallbladder and bile ducts.
Cholelithiasis-formation of stones or calculi. May not create symptoms until or unless gallbladder or duct becomes blocked and inflamed.
May attempt to reduce inflammation with antibiotics first.
Another treatment may be oral bile acids or extracorporeal shockwave lithotripsy.
Pancreatitis-Acute or chronic inflammation of the pancreas. Biliary tract disease and alcoholism along with drugs, estrogen use, infection, hypertriglyceridemia, and structural abnormalities are main causes. Pain is severe. Persistent vomiting occurs. It may quickly become very ill and unstable. It can lead to shock, systems failure and death. Refer to your textbook pg 343
Related medication and treatment: Refer to your textbook pd 344
Treatment of acute vs. chronic may vary according to symptoms.
Supportive therapy including hyperalimentation and intravenous therapy. Relief of symptoms including nausea, vomiting, abdominal tenderness and acute pain.
Monitor for hypotension, urine output, and hypoxemia.
Oxygen
Antibiotics (for specific infections-biliary sepsis, pulmonary infections, UTI)
Dietary restrictions
H2 blocker or antacids
Pancreatic enzymes (inhibit release of cholecystokinin)
Enteritis-inflammation of the intestine. Many forms of gastrointestinal enteritis exist, depending on the location and source of inflammation-medications, bacteria, viruses, fungi, food allergies, parasites.
Related medication and treatment:
Supportive treatment is most important.
Easy access to toilet.
Anti-emetics
Oral fluid replacement or IV fluids.
Suppositories may be used as route of medication administration if diarrhea is not present or profuse.
Crohn's disease-also known as regional enteritis, granulomatous ileitis or ileocolitis (nonspecific inflammation of the distal ileum and colon). May have a genetic propensity. Refer to your textbook pg 343
Video on living with Crohn's disease and signs and symptoms: Click Here
Related medication and treatment:
Supportive care may include oral anticholinergics, bulking agents (psyllium preparations), sulfasalazine, antibiotics, corticosteroids (prednisone, hydrocortisone).
Corticosteroid-budesonide can be given orally or as an enema.
Other drugs such as methotrexate may be given.
Surgery may be necessary for recurrent intestinal obstruction or abscesses.
Ulcerative colitis-chronic inflammatory and ulcerative disease in the mucosa of the colon, characterized by bloody diarrhea. Unknown cause; bleeding is the most common complication along with toxic colitis progressing to dilation of the colon, loss of muscle tone. Refer to your textbook pg 343
Related medication and treatment:
Diet can be important-avoiding raw fruits and vegetables, limits the mechanical trauma to the inflamed colon.
Anti-cholinergic drugsor loperamide (Imodium) may be used.
Medication for treatment of diarrhea must be used with caution to avoid toxic megacolon (relaxation, dilation of the colon).
Hydrocortisone enemas may be given.
Mesalamine may be given by enema or suppositories. Other treatment may be similar to treating Crohn's's disease.
Peritonitis-inflammation of the membranous coat lining the abdominal cavity. Infectious agent gains access through a rupture or perforation of the bowel or organ or carried by blood stream or lymphatic vessels. Refer to your textbook pg 344
Related medication and treatment:
Treatment for mild infection is antibiotics.
Surgery may be necessary for perforated bowel, stomach, and appendix.
Irritable bowel--A non-inflammatory disorder of the intestine characterized by abdominal pain, constipation, diarrhea, abdominal bloating, and passage of mucus. Cause is unknown. Emotional factors, diet, drugs, or hormones may aggravate Gl motility. Organic disease may be present, or in addition fibromyalgia, headaches, temporomandibular joint (TMJ) syndrome, hypothyroidism. Refer to your textbook pg 344
Related medication and treatment:
Supportive treatment includes psychological support, empathic care, reduction in external stressors, regular physical activity.
Anti-cholinergics (antispasmodics) may be used in addition to fiber.
Loperamide (Imodium) may be used when resident has diarrhea.
Antidepressants may relieve constipation and bloating (by down regulating the activity of spinal cord and cortical afferent pathways from the intestine).
Aromatic oils (carminatives) can relax smooth muscle and relieve pain (peppermint oil).
Normal diet usually followed, but individuals may benefit from reduction or elimination of beans, cabbage, other foods containing fermentable carbohydrates; reduced intake of apple, grape juice, bananas.
Artificial sweeteners such as sorbitol, mannitol, fructose may be avoided.
Increase in dietary fiber, bland bulk-producing agents may be administered (bran, psyllium). Avoid excessive use of fiber which can lead to bloating and diarrhea
Diverticulosis-disease caused by sac-like mucosal projections in the GI tract which cause symptoms by trapping feces, becoming infected, bleeding, or rupturing. Related to segmental spasm of the muscular coat of the bowel, increased pressure causing extrusion at the weakest points of the muscle layer. Refer to your textbook pg 344
Related medication and treatment:
Treatment involves reducing spasm.
Diet high in roughage may help along with psyllium and bran.
Antispasmodics don't always help. Chronic use in elderly can cause more problems.
Surgery is sometimes indicated.
Diverticulitis-inflammation of the mucosa with complications such as abscess, peritonitis, obstruction, fistulas, bleeding. Usually there is pain, local tenderness in left lower quadrant of the abdomen and fever. Complications may occur, obstruction, fistulas.
Treatment in mild cases includes rest, liquid diet, oral antibiotics (Cephalexin).
With improvement, diet may advance to soft low-roughage and daily psyllium.
Once resolved, high-roughage diet resumed.
Severe symptoms or with other complications, may require IV antibiotics and surgery
Hemorrhoids-Dilated veins in the anal-rectal area. Refer to your textbook pg 344
May be external or internal to the anus, may protrude.
May regress spontaneously or be reduced manually.
Hemorrhoidal bleeding typically follows defecation.
Thrombosed or ulcerated hemorrhoids are painful.
Pain can be severe.
Internal hemorrhoids may cause a feeling of incomplete defecation.
Examining the rectum after straining at defecation will usually determine if there are hemorrhoids.
Itching of the anal area is not usually related to hemorrhoids.
Related medication and treatment:
Treat with stool softeners, bulking agents (psyllium), warm sitz baths, anesthetic ointments, or witch hazel compresses.
Large or protruding hemorrhoids may require surgery.
Parasites-Parasites are organisms that grow, feed and are sheltered on or in a different organism. Refer to your textbook pg 344.Protozoans may live outside or inside the intestines. Entamoeba histolytica ("Montezuma's revenge"), Giardia lamblia, Cryptosporidium, and Cyclospora are some of the more common intestinal parasites. Intestinal protozoa are passed by the fecal-oral route. Common in developing countries with poor sanitation, locations where there is fecal incontinence and poor hygiene (persons who are incapable of performing hygiene correctly-very young, elderly, or mentally incompetent). Some may be spread through sexual contact. Person may be asymptomatic but spread disease to others. Prevention involves good hand-washing, preventing contamination by fecal matter. Symptoms may include watery malodorous diarrhea, abdominal cramps and distention, flatulence, intermittent nausea, chills, head ache. Stool cultures may be necessary to diagnose and correctly treat.
Related medication and treatment:
Antiparasitics-given to kill worms (parasites also known as "helminths").
Oral metronidazole (Flagyl) is effective for Giardia.
No specific treatment is effective in Cryptosporidium-prevention of contamination is key.
Double strength oral trimethoprim-sulfamethoxazole(Bactrim, Septra) for isosporiasis and cyclosporiasis.
Additional GI-related medications and treatments:
Antacids-relieve gastric and ulcer pain; neutralize stomach acid. Treat hyperacidity, peptic ulcer, gastritis, and indigestion. Refer to your textbook pg 344-345
Sodium bicarbonate (baking soda).
Calcium salts-seldom used.
Aluminum salts (Amphogel, Rolaids).
Magnesium salts (Milk of Magnesia)-MOM dose determines its use: 30 cc is a laxative; 5 cc is an antacid.
Combination of Mg and aluminum (Maalox, Mylanta, Gelusil, Aludrox, Riopan)
Nursing care and side effects:
These drugs interfere with the absorption of all other drugs, so should not be given at the same time as other medications. Administration at 30 minutes before or after other drugs.
Effect is prolonged when taken with food.
Persons with heart and kidney problems on sodium restricted diets should not take sodium bicarbonate. It is not safe for long-term use, can change the blood to a more alkaline level, and cause heart rhythm problems.
Calcium salts-constipating.
Aluminum salts-constipating.
Magnesium salts-cause diarrhea.
Combination products, magnesium and aluminum are used to balance out the constipating and laxative effects of each other.
Anti-secretory-help inhibit gastric acid secretion by reducing the amount of histamine (H,), a chemical which stimulates the formation of stomach acid. May be used in treating ulcers, hyperacidity, and avoiding irritation of the stomach when gastrostomy tube is placed. Peptic ulcer disease is no longer believed to be primarily due to hyperacidity. More knowledge is being gained about H. pylori, a pathogen believed to be a causative factor in acid-peptic disease. NSAIDs and the breakdown in the mucosa of the stomach are also contributors. Refer to your textbook pg 345
Cimetidine (Tagamet)
Omeprazole (Prilosec)
nizatidine (Axid)
ranitidine (Zantac)
famotidine (Pepcid)
lansoprazole (Prevacid)
esomeprazole (Nexium)
Nursing care and side effects:
May cause headache, abdominal pain, nausea, vomiting, and diarrhea.
Should be taken before meals.
Digestants--help promote digestion, replace or supplement naturally produced digestive juices. Stimulate production of digestive fluids, treatment for digestion for chronic pancreatitis, milk intolerance (lactose sugar). Refer to your textbook pg 346
GI upset--do not give with antacids without doctor's permission.
Monitor resident's response to these supplements.
Anti-flatulents-reduce gas production by mildly stimulating motility or gathering bubbles of gas together so they can pass more easily. Reduces the feeling of gassiness and bloating, particularly in indigestion. Taken as a preventative or given following abdominal surgery to prevent postoperative bloating from immotility. Refer to your textbook pg 346
Simethicone (Mylicon, Max Strength Phazyme, Maalox Anti-Gas, Mylanta Gas Relief)
Nursing care and side effects:
Dietary modifications may be necessary once foods which produce gas are identified for the resident.
Encourage resident to chew food thoroughly.
Medication should be given after meals and at bedtime for best results.
Chewable tablets should be chewed thoroughly before swallowing.
Antiemetics-suppress nausea and vomiting by acting on the control center in the brain. Used for motion sickness, nausea associated with chemotherapy, and nausea caused by drugs. Most are antihistamines and phenotbiazines (tranquilizers). Refer to your textbook pg 347
Dimenhydrinate (Dramamine)
Trimethobenzamide (Tigan)
Meclizine (Antivert)
Phenotbiazines (Compazine, Thorazine, Phenergan)
Marinol--derived from marijuana.
Nursing care and side effects:
• Most cause drowsiness, dizziness and postural hypotension (risk for falling).
Anti-cholinergics-slow down peristalsis and intestinal motility by blocking the action of acetylcholine (the chemical that transmits nerve impulses at the synapse). Less acid is produced in the stomach; alkaloids. Used for ulcers, irritable bowel syndrome, spastic colon, and diarrhea. Refer to your textbook pg 348
Atropine sulfate and diphenoxylate HCL (Lomotil)
Atropine, scopolamine, phenobarbital (Donnatal)
Kaolin, pectin, atropine, belladonna (Donnagel)
Loperamide (Imodium)
Banthine
Pro-Banthine
Nursing care and side effects:
Side effects vary according to the type of medication. Many are due to stimulation of the parasympathetic nervous system causing blurred vision, dilated pupils, dry mouth, heart palpitations, constipation, and urine retention.
Observe for side effects.
Replace fluids.
Rest the intestines (limit solid foods).
Antispasmodics-act on the smooth muscle in the intestines and stomach. May be combined with anti-cholinergics. As with most anti-cholinergics, use in the elderly may be contraindicated because of other disease processes (glaucoma, heart disease, bladder dysfunction, obstructive diseases).
Dicyclomine hydrochloride (Bentyl)
Atropine, scopolamine, phenobarbital (Donnatal)
Hyoscyamine (Levsin)
Nursing care and side effects:
Side effects vary for each medication. Many are similar or the same as those for anti-cholinergics (dryness of mouth, heart palpitations, urine retention).
Most are contraindicated and should not be given to residents who have glaucoma.
Diarrhea medications-drugs used to relieve diarrhea; absorb fluids, decrease intestinal motility, shrink swollen tissue, or coat and soothe tissues. Refer to your textbook pg 348
Kaolin
Bismuth (Pepto-Bismol)
Pectin
Kaolin and pectate combination (Kaopectate)
Camphorated opium tincture-paregoric
Loperamide (Imodium)
Nursing care and side effects:
Some medications cause drowsiness. Many anti-diarrhea medications are also anti-cholinergics.
Risks associated with misused.
Replace fluids and rest intestines. Non-drug means of treating diarrhea include limiting solid food intake. Fluids may be limited for short periods of time.
Eliminate foods that may stimulate diarrhea.
Observe for symptoms of dehydration and report to licensed nurse.
Emetics - used to produce vomiting in cases of poisoning. Refer to your textbook pg 346-347.
Syrup of ipecac
Cathartics (laxatives and purgatives)-promote defecation through various actions. "Laxatives" are more slow-acting and gentle and may be used as a preparation for bowel and rectal exam, constipation, and stool softener. Purgatives are used to thoroughly clean intestinal tract in preparation for surgery or diagnostic testing. They may also be used in treating constipation. Refer to your textbook p 314
Stimulant-castor oil (Neoloid), senna (Senokot), bisacodyl (Dulcolax), phenolphthalein (Dialose Plus, Ex-lax). May cause cramping.
Saline cathartic-magnesium hydroxide (Milk of Magnesia"MOM") in large dose, Epsom salts.
Bulk former-draw fluids into feces. Increased volume stimulates peristalsis. Fortify with additional fluids during the day. Few side effects. Psyllium (Metamucil), psyllium without sugar (Konsyl).
Lubricant-lubricate the feces. May interfere with absorption of some vitamins. Not given with food or meals. Mineral oil.
Emollient-moisten and soften feces; non-irritating but take longer for action. Dioctyl calcium sulfosuccinate (Surfak), dioctyl sodium sulfosuccinate (Colace), docusate sodium (Colace), combination with mild laxative (Peri-colace).
Nursing care and side effects:
Preventing constipation includes providing a diet that is high in fiber and fluids and regular exercise.
Dependency on laxatives or purgatives may alter the resident's bowel habits.
Changes in bowel habits can be an indication of more serious problems such as a bowel obstruction.
Residents should always be assured ready and safe access to toileting when cathartics are given. It is not reasonable to expect a resident to "wait" or "hold it”. Some residents may have urgent need for emptying. Losing control of bowels is both dangerous for the resident and humiliating.
All nursing staff should be alerted if resident is given a cathartic medication. The resident's usual bowel habits should be identified.
Observe for cramping, rectal bleeding, nausea or vomiting; report to licensed nurse.
Refer to your textbook pg 353 diagram 12.1 for OTC Medications for Gastrointestinal Disorders
Pay close attention to your textbook pg 356-360regarding Representative Drugs for the Cardiovascular System
Also read the in your textbook pg 356-360 the practice procedure for administering medication through a nasogastric or gastrostomy tube. Refer to Giving Gastrointestinal Medications in your textbook pg 353.
Use your browser's "Back" button to go back to course documents
Please view the Powerpoint slide show on Drugs for the Gastrointestinal System.
Don’t forget to participate in the discussion board topics 4-6 for Unit 2 if you have not yet done so.
Use your browser's "Back" button to go back. You may go to the “Lab” tab and play games as a learning tool. If the games do not work initially, you may try a new browser than what you currently are on. Try Internet Explorer, Safari, Firefox, or Google Chrome to name a few.
 Unit 13
Unit 13